
“For a small practice, it is more critical to embrace MACRA sooner, to avoid the negative impact on your income.”
- Jas Grewal, CEO at CareSkore
We took the pain of reading through the 962 page MACRA NPRM document to understand the intricacies of the law.
The good news: MACRA will pay physicians for doing what they already want to do: provide the best possible care for their patients. Hence when a provider does the best thing in the interest of the patient — doing good — they’ll also do financially well.
The bad news: MACRA is soon to be a reality. Experts are calling it the most significant change to clinician reimbursement in more than two decades. And that means you have to be ready.
Fast and Furious
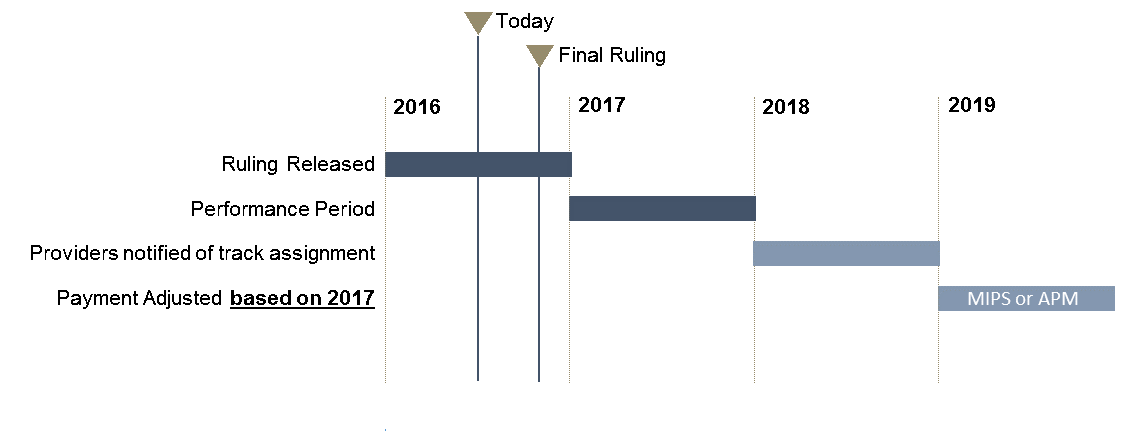
The MACRA timeline is aggressive—performance measures go into effect in 2017—and you need to get up to speed on how this complex program will impact your organization.
You have to start now, to ensure implementation of tools needed to baseline your performance and jumpstart the MACRA journey. MIPS payments start in 2019, based on the quality of care starting with 2017. Hence, 2016 an important year for you to understand and strengthen quality benchmarks.
So what should a clinician do as far as technology is concerned?
By 2017, the clinicians should
- Use a 2014 or 2015 Edition Certified HER
- Decide which track they should choose when reporting to CMS
- Report on stage 2 or stage 3 care information objectives and measures
- Allow ONC to review of their EHR; provide support for HIE
And, when they get spare time after that, continue to take care of their patients
MACRA Implementation Timeline
Financial Impact & Incentives
A major question is how aggressively the MIPS program would redistribute payments from low performers to high performers.
As we combed through the enormous document, we found that CMS’s analysis estimates the impact on providers by practice size in Table 64 (Page 676 of 962), suggesting that 87% of eligible clinicians in solo practices and 70% of practices with two to nine clinicians will have a negative adjustment due to a below average score.
These estimates suggest that in the first year, the average MIPS adjustment (positive or negative) would be several thousand dollars per clinician.
Clinicians working for a practice with 100 or more eligible clinicians, 81.3% will have a positive adjustment, only 18.3% are estimated to receive a negative adjustment.
In total, the solo physician practices with a negative payment adjustment would collectively be getting $300 million less than they would without MIPS. This number is only $57 million for practices with 100 or more eligible physicians.
Small Providers
If you are a clinician or group that fall under the low volume threshold that CMS defines as clinicians or groups with $10,000 or less in Medicare charges AND 100 or fewer Medicare patients or in first year billing Medicare, you are excluded from MACRA.
That is only a tiny fraction of the providers.
Smaller providers face steep challenges complying with MACRA metrics, in particular, the EHR and technology-based requirements or some of the qualifying APMs that require greater capital or a patient population.
MACRA will enable provider affiliations will be characterized by tight partnerships through which the entities can share capabilities.
Smaller, independent practices may actually have more agility as the sole authority in crafting their MACRA strategy. Independent medical groups have will have more flexibility in what they do to respond to MACRA that medical groups associated with hospitals or health systems won’t have.
Looking Forward
Final MACRA rules are still a couple of months away, and there could be some change in the ruling. However, the proposal gives insights on CMS’s thought process and what to expect with final ruling later this year. Not only the regulatory reporting is going to be substantial, but also the financial incentives are significant. Hence, the clinical and financial outcomes of your practice are very co-related as MACRA gets into effect.
As provider’s address MACRA, they need to address not only MIPS/APMs, but also Medicare Advantage, Medicaid incentives, and commercial insurances. Stay tuned for future posts as we address these concerns.
References
- The MACRA proposed rule is at: https://www.gpo.gov/fdsys/pkg/FR-2016-05-09/pdf/2016-10032.pdf.
- The CMS “Measure Development Plan” is at: https://www.cms.gov/Medicare/Quality-Initiatives-Patient-Assessment-Instruments/Value-Based-Programs/MACRA-MIPS-and-APMs/Final-MDP.pdf.