
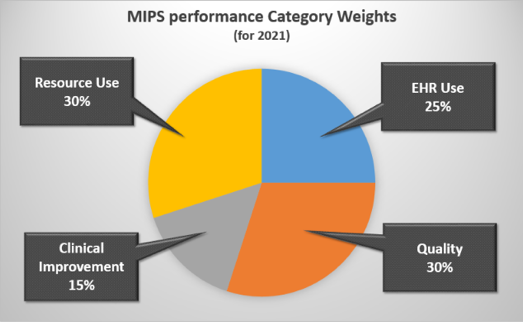
Under the MACRA, providers will be reimbursed according to a composite score that reflects how well you’re providing value-based care. This composite score comprises of four key categories: the quality of care you provide, the efficiency of your resource use, meaningful use of EHR, and last but certainly not least, clinical practice improvement activities (CPIA).
A rising tide lifts all boats, right? The great part about MIPS—one of the two payment programs as part of MACRA—is that all of these metrics tie-in to improve clinical outcomes and patient engagement. This leads to cost savings, efficient resource use, and improved adoption of your EHR. Maximizing your composite score will not only affect your payments positively, but it will help you provide efficient patient care.
Not all activities are created equal
Certain categories are worth more than others due to their impact on patient care. High-weighted activities are worth 20 points, whereas medium-weighted activities value at 10 points. While these CPIAs only account for 15% of your total score, leveraging the highest-weighted tactics can be easy wins for your practice. Planning, completing and reporting 3 activities is much easier to pull off than 6 different initiatives. During your 90-reporting period (here’s a plan for when should start thinking about it), you must achieve 60 points by completing these clinical practice improvement activities in which there are over 90 tactics across 8 categories, in the combination of your choice.
Here’s a look at some of the types of activities in each category per ASCRS:
Expanded Practice Access: expanded practice hours, telehealth services, and improving access to services
Population Management: chronic care management programs, community and rural healthcare programs
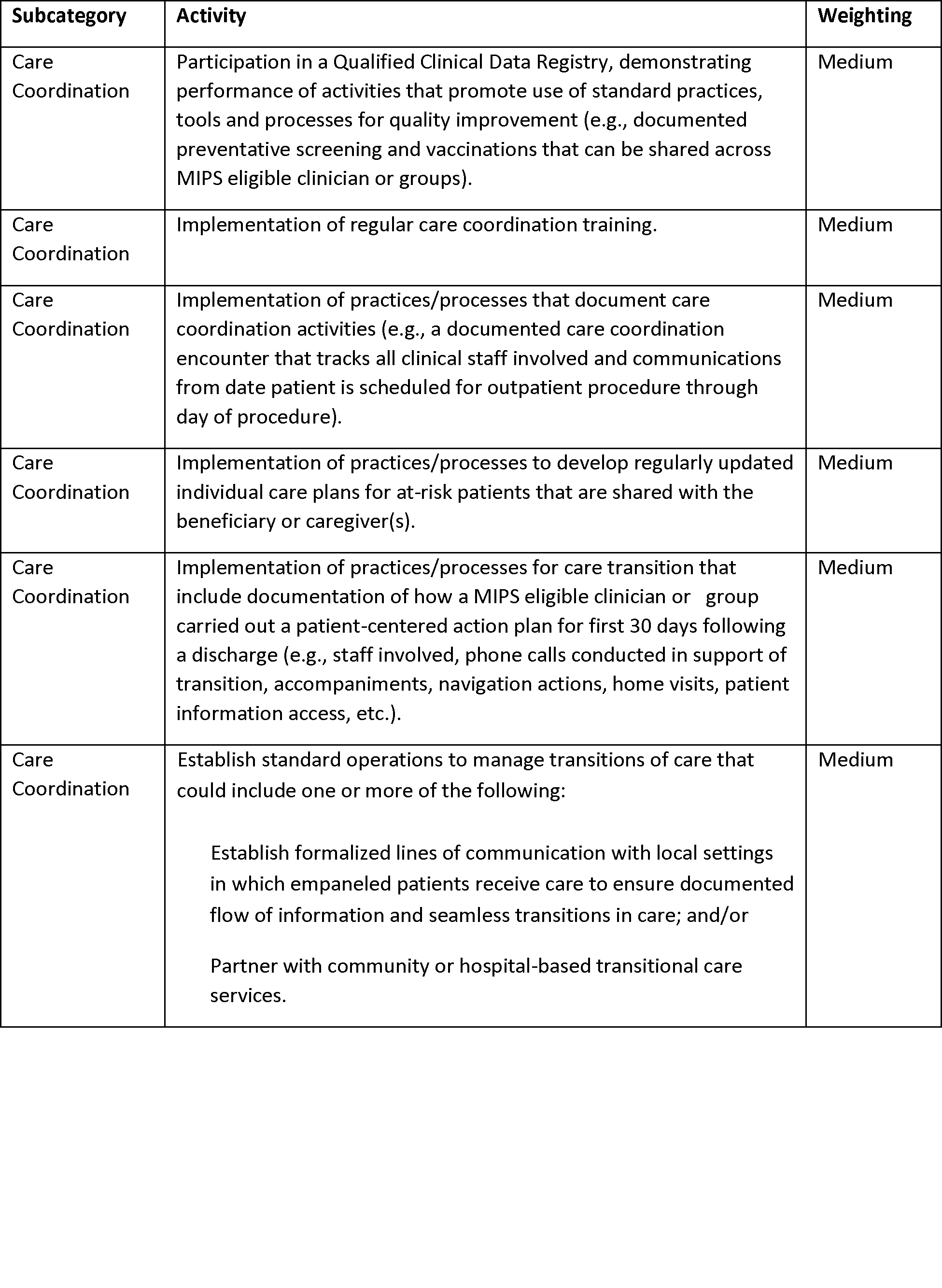
Care coordination: health information sharing, timely communication and follow-up, care coordination training to handle transitions of care, and active referral management
Beneficiary Engagement: EHR to document patient-reported outcome,enhanced patient portals
Patient Safety and Practice Assessment: ongoing practice assessments and patient safety improvements, and use of tools such as the Surgical Risk Calculator
Achieving Health Equity: seeing new and follow-up Medicaid patients in a timely manner, and use of QCDR for demonstrating performance of processes for screening for social determinants
Emergency Response and Preparedness: participate in disaster medical teams or participation in domestic or international humanitarian volunteer work
Integrated Behavioral and Mental Health: tobacco intervention and smoking cessation, and integration with mental health services.
Choosing your activities
With several ways to maximize points in these categories, many activities may overlap and will have a bigger benefit for your patients.
Let’s take the Beneficiary Engagement and Population Management categories for example. You can implement specific programs and protocols to help patients with chronic illness like heart disease and diabetes. Helping patients manage their care at home with blood pressure testing and glucose measurements will help keep them on track and reduce the risk of readmission.
Bonus: Have a tool where patients can electronically share data and communicate with providers.
Convenience is king
Anything you can do to make life easier for your patients will most likely be a highly weighted CPIA. Expanding access to care with extended hours or e-visits can significantly decrease appointment cancellations or no-shows. Also, providing 24/7 real-time communication with care teams and reminders will greatly improve patient engagement and overall outcomes.
Another highly weighted activity is participation in CMS’s Transforming Clinical Practice Initiative which aims to help:
- Exchange patient data information for the best continuity of care
- Track patients through the entire process and integrate information from specialists to make sure care is documented
- Coordinate phone calls, communication, navigation post-discharge
- Communicate timely results for follow-up
- Create individualized care plans for high-risk patients to share with other providers
Attaining Full Credit with Reporting
Given that the entire healthcare industry is shifting towards value-based care, reporting will be one of the most critical components within the continuum of care. If you haven’t already, begin to determine what measures you will report on and evaluate your strengths. Identify what gaps can be filled and put in the necessary plans to improve those gaps. Here at CareSkore, we envision providers getting the credit they deserve.
Through CareSkore, providers can:
- Generate reports for measures including MACRA, PQRS, and HEDIS
- Manage your patient population with real-time assessments
- Understand patient data and quality metrics in order to improve outcomes
Whether it’s reporting for Clinical Improvement Activities or any of the mentioned categories, understanding your patient population through reporting is the first step to cultivating the provider-to-patient relationship.
Sources:
MIPS, MACRA & MU - The Next Evolution of Healthcare Payment Reform
MIPS: Clinical Practice Improvement Activities Category
MIPS Program: 2017 Clinical Practice Improvement Category Proposed Rule Guide
Federal Register - Subcategories
Medicare Program; MIPS and APM Incentive Under the Physician Fee Schedule
Transforming Clinical Practice Incentives

{kind=link}